The Locked-in Syndrome: Living A Prisoner Of One’s Own Body

Locked-in syndrome, or motor derefferentation syndrome, is an infrequent condition caused by pontine lesion in the brain. The repercussion of the lesion of the bridge is very serious and leads the person being victim to not being able to move his body any more, except the eyes and the eyelids. However, even if she loses almost all of her motor skills, her consciousness as well as her somatosensory system remain intact.
It is as if the brain “disconnects” from the body and loses its ability to give it orders. However, it continues to receive all sensitive signals such as pain and temperature, but also somatic signals such as hunger. Communication becomes almost impossible given the inability to move the phonatory muscles, and it remains relegated to the use of eyelid movement.
In some cases, a form of communication has been established through the blinking of the eyelids. With a panel where the letters of the alphabet appear, the person will choose the letters of the words and sentences he wants to form. It is a slow method but which could “give voice” to those who have lost the use of speech due to this syndrome.
The symptomatic framework of this pathology is: quadriplegia, anarthria (inability to articulate words) and conservation of consciousness. Since the cerebral cortex and thalamus are not affected, cognitive functions are not either. The subject perceives, processes and produces information normally through the use of cognitive processes. He is able to perceive all external stimuli, but cannot respond to them physically.
The main cause is basilar thrombosis, the precursor symptoms of which can be seen in the weeks or even months before the onset of the syndrome, such as dizziness or nausea. There are also non-vascular causes such as traumatic brain injury, with contusion of the brainstem or by vertebrobasilar dissection. Depending on the severity of the motor engagement, we can distinguish three clinical settings:
- Classic: quadriplegia and anarthria with preservation of consciousness and ocular motility or fluttering of the eyelids.
- Incomplete: Similar to the classic clinical setting, but retaining one movement more than eye movement.
- Total: without the preservation of any movement, is usually accompanied by lesions in the midbrain.
Depending on its course, the syndrome can be transient or chronic. Even in cases where disconnection of downlink voices from the bridge has been observed, recovery is not possible. Disconnecting the descending pathways means that orders sent to the rest of the body do not arrive, and as a result, the body cannot respond to any stimulation, even if it receives them.
It makes sense to think about the difficulty of detecting locked-un syndrome and differentiating it from others, such as coma. In fact, in the first place, it is not easy to know if the mental faculties of the patient are intact, since they cannot communicate.
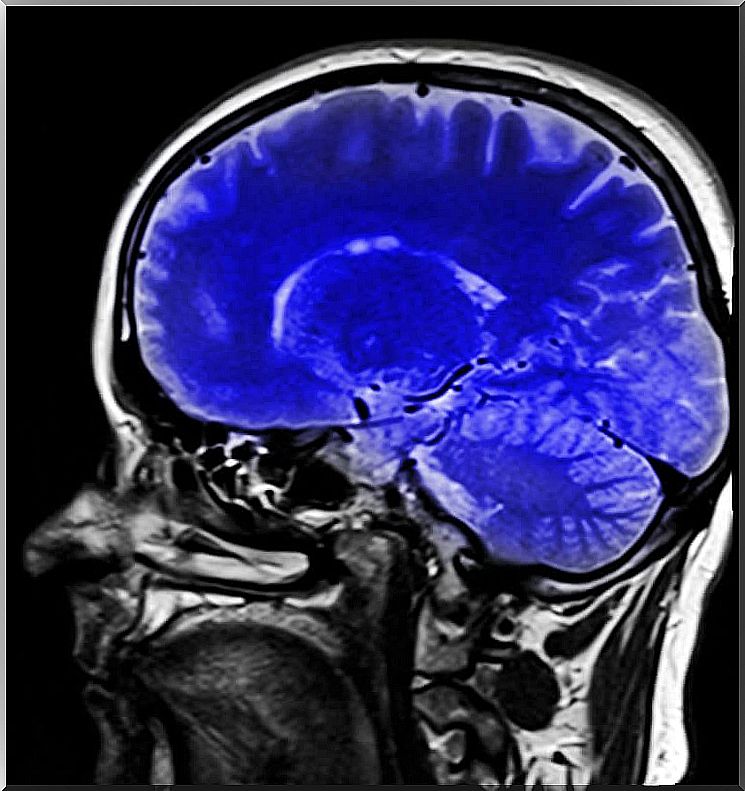
There are neurological tests that help make a diagnosis. MRI can show the type of brain injury that may or may not point to a diagnosis of locked-in syndrome.
Both positron emission tomography (PET) and electroencephalogram (EEG) can provide information on brain activity. Through the PET, we can observe if the brain metabolism is normal, and if so, it would mean that the brain functions are preserved and that there is awareness of the syndrome.
Through EEG, we can monitor brain wave activity. Thanks to a few electrodes placed on the head, this tool makes it possible to determine the waves which predominate at the moment. In the case of a person suffering from locked-in syndrome, a reactivated posterior alpha rhythm would be observed.
Jean-Dominique Bauby was a French journalist. At 43, he suffered a cerebral embolism. After being in a coma for 20 days, Bauby came out of it, but with locked-in syndrome; he was only able to move his left eye then, and his head slightly. He suffered from a great physical deterioration, and by then had lost 27 kilos in a few weeks.
His health was getting worse as a result of the embolism he had suffered. He then lived with the disease for about a year, during which time he was “locked in his own body”. He learned a method of communicating, with an alphabet panel and through the blink of an eye. With the help of speech therapists and his family, he wrote an autobiographical book called The Butterfly and the Diving Bell, which was a huge success.
There is also a film based on his book of the same name, where we can observe the challenge that Jean-Dominique Bauby poses to face this harsh illness and the thoughts that haunt his mind that his body is not capable of. Express. He uses the imagination and he “travels” through his mind to different places that allow him to escape a reality that is difficult to face.

We all know what physical stillness is, but what about mental stillness? It seems more complicated to perceive and solve.